This is the first in a series of blog posts on this topic. In this blog, I will share some thoughts on where transportation obstacles may pose a barrier to individuals, particularly in rural areas, becoming vaccinated.
First and foremost, people will need to choose to be vaccinated. This is not an easy feat. The creation of these vaccines happened at lightning speed, in a matter of months versus the four or so years it usually takes. In addition, the vaccination development has been somewhat tainted by perceptions that is has been politicized, leading to some distrust in that process.
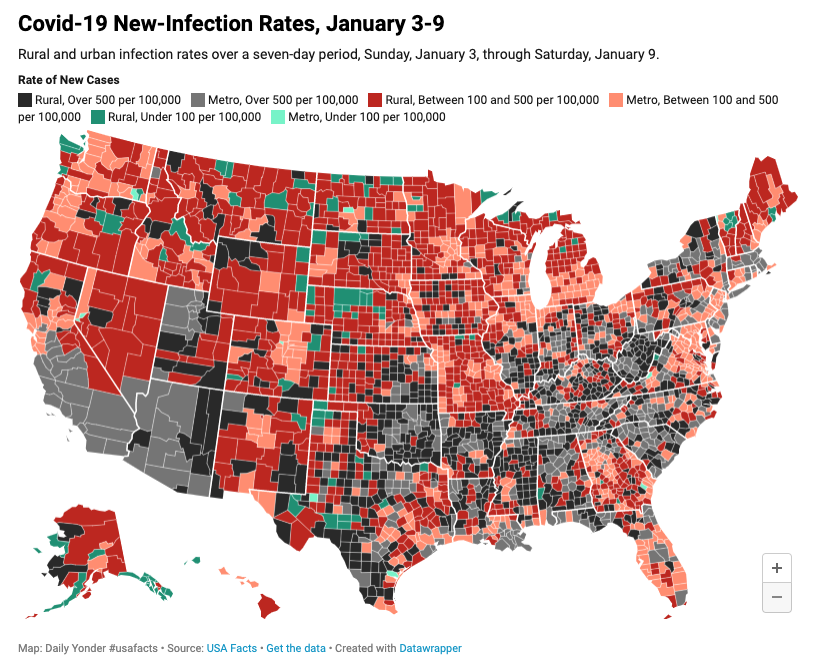
A January 2021 poll by the Kaiser Family Foundation noted that 35% of rural respondents indicated they probably or definitely would not get the vaccine. Consider this in the context of reporting from nonpartisan Center for Rural Strategies that the rate of new cases in rural areas is skyrocketing. I have also heard anecdotally of rural transit drivers imploring their bosses, “Don’t make me get the vaccine, please.” There are ways to help people understand the new vaccines, such as this CDC toolkit found here.
Choosing to be vaccinated against COVID-19, as with other vaccines, will remain a personal choice. But for those who do want to be vaccinated, what transportation-related barriers will stand in their way? A professor from Binghamton University synthesized some of the challenges earlier this month. In addition, I am hearing the following:
- Older adults may be too scared to leave their homes to be vaccinated, as they fear this will expose them to the vaccine before they develop immunity.
- Older adults and those who do not drive have no way of getting to vaccination sites. This is one of the raison d’être for rural demand-response transportation; if rural transportation services are vital to these residents getting to health care appointments, pharmacies, and grocery stores, then they are equally crucial for transportation to vaccination sites.
- We know that the recent trend has been for rural health care facilities to be closed and/or consolidated into more urban areas. This could mean rural populations have to travel even further to be vaccinated.
Also, one needs to consider the efficient use of all doses of vaccine in one vial. The Pfizer vaccine (the one that needs to be kept at very cold temperatures), has approximately six doses in each vial and requires two vaccinations to achieve maximum immunity. The Moderna vaccine has approximately ten doses in each vial which also requires two vaccinations to achieve maximum immunity. (The third vaccine, developed by AstraZeneca, has not yet been approved for emergency-use in the U.S.). This means, that depending on which vaccine a rural clinic has, it will need to carefully schedule the number of recipients so there are no leftover doses as well as keep and transport the vials at optimal temperatures; the vaccine cannot be re-frozen once the vial is opened.
Rural transit’s role can encompass several activities. FTA has recently published this FAQ, CE18: Are FTA funds available to provide transportation to or from COVID-19 vaccination site? addressing what is allowable under CARES and Coronavirus Response and Relief Supplemental Appropriations Act of 2021(CRRSA) funds.
Here are a few ideas floating in the field:
- Help in distributing information on the vaccine. This can be done in conjunction with local senior services organizations, rural health clinics, etc. Many rural drivers have developed ongoing relationships with their regular riders and may be seen as trusted conveyors of information.
- Providing fare-free rides for community residents to regional vaccination sites
- Adapting a transportation hub as a vaccination site
- Using transit buses as mobile vaccination clinics
- If one location runs out of the vaccine, providing transportation to an alternative site
- As demand-response systems bring individuals to vaccination sites, scheduling patients’ second vaccination ride at the same time to ensure they receive both doses of the vaccine
Finally, here are just four examples of transportation initiatives, both public and private, we have gathered:
- Lawrence County, NY has designated five main clinics for shots for vaccine appointments. In addition, the county will coordinate with its hospital partners to create “site-specific” clinics to vaccinate eligible people who have difficulty with transportation.
- Meaford, Ontario, Canada: A partnership with the Bruce and Grey Counties and the local school transportation consortium provides access to both large and small vehicle fleets with the capacity to achieve the desired immunization target.
- Uber has committed to providing 10 million free and discounted rides to help “ensure transportation is not a barrier to getting a vaccine.”
- Lyft has partnered with health insurance giant Anthem, JP Morgan Chase and the United Way among several other groups and companies to get Americans to and from Covid-19 vaccination sites. When Covid-19 vaccinations are available to the broader public, Lyft’s ride share network will be prepared to transport 60 million low-income and uninsured Americans to vaccination sites.
See more examples here and by searching “coronavirus” on NCMM’s website. As your role vis-à-vis vaccination evolves, please let us know so we can add you to our table.